


All Global Research articles can be read in 51 languages by activating the “Translate Website” drop down menu on the top banner of our home page (Desktop version).
To receive Global Research’s Daily Newsletter (selected articles), click here.
Visit and follow us on Instagram at @crg_globalresearch.
***
The FDA has refused to even explore approval of cheap, safe, and effective repurposed drugs for 20 months, despite mounds of evidence from studies vouching for their efficacy and safety. So, naturally, now that the agency is on track to issue an emergency use authorization to the first outpatient drug for COVID, this one must be the greatest thing since penicillin, right? Wrong! In fact, the drug is so dangerous and has so many known and unknown side effects that the FDA advisory committee members basically admitted this was a “difficult” decision and that they could rescind the authorization later on. This decision makes their rejection of ivermectin, fluvoxamine, nitazoxanide, and hydroxychloroquine all the more indefensible.
If you liked remdesivir, you will surely like Merck’s molnupiravir, which was developed with the help of the same entities guarding its approval based on flawed data produced by the company itself that is making over $1 billion off the federal government. No conflict of interest whatsoever!
Although the fix was in because no drug produced by Merck or Pfizer – no matter how dangerous – will ever be turned down, the approval was as revealing as it was appalling. The fact that the vote even by these compromised hacks was 13-10 demonstrates just how problematic molnupiravir likely is out of the gate.
Yesterday, the FDA’s Antimicrobial Drugs Advisory Committee voted 13-10 to approve molnupiravir at 800 milligrams twice a day for five days of COVID treatment for people in at-risk categories. It still needs official approval from the FDA and the CDC before it can be used, but the fix has long been in.
As CNBC reports, even those who voted for the drug admitted that it was a difficult decision and asked to revisit the authorization down the road. They conceded, as I have warned, that this drug can be mutagenic and cause birth defects, in addition to the fact that Merck’s own manipulated data show the efficacy is very modest.
“Given the large potential population affected, the risk of widespread effects on potential birth defects, especially delayed effects on the male, has not been adequately studied,” warned Dr. Sankar Swaminathan, an infectious disease specialist at the University of Utah School of Medicine, who voted no.
As CNBC reports:
The FDA and Merck both recommended against using the drug in kids and pregnant women. Molnupiravir was found to be lethal to embryos in pregnant rats, also causing birth defects and reducing fetal body weight. It also caused other defects that interfered with bone growth in young pups, along with other abnormalities, the data shows.
Just like the vaccines and remdesivir, this drug hits the triple crown – fails on efficacy, causes injury, and also induces mutants and viral escape, possibly making the virus worse. In the FDA’s briefing document on the drug for yesterday’s meeting, it states clearly that “there are potential safety concerns pertaining to MOV, including embryofetal toxicity, bone and cartilage toxicity, and mutagenicity.” They also observe that there is evidence molnupiravir “may increase the rate of changes in the viral spike protein, which, in theory, could enhance SARS-CoV-2 spike protein evolution.”
“Of particular interest, in some participants, MOV treatment was associated with amino acid changes at sites/regions of spike that are likely under immune or other evolutionary pressure,” warns the onetime gatekeeper that has now become a collaborator with Big Pharma. This sounds an awful lot like Dr. Geert Vanden Bossche’s warning about the vaccines placing evolutionary pressure on the virus, which likely resulted in making it more durable this year than in 2020. “Collectively, these analyses indicate MOV treatment may increase the rate of emergence of SARS-CoV-2 populations with amino acid changes in the viral spike protein, consistent with its mutagenic mechanism of action,” warns the FDA.
Nonetheless, Dr. Michael Green, a pediatric transplant specialist at University of Pittsburgh School of Medicine Division of Infectious Diseases, said the lack of available therapies swayed him and others to vote to approve the drug.
The problem is that after incurring such unknown risk for a drug that has never succeeded and has known safety problems, the efficacy is very modest. Even Merck’s own trial shows barely any efficacy for Delta, and we all know by now how reliable the data can be from the manufacturer itself!
The FDA approves Molnupiravir by 13 votes to 10.
If you're hit by Delta, Merck's trial data show with a 95% confidence that your risk of hospitalization or death is:
• reduced by 7.8% or increased by 2.9% (absolute)
• reduced by 57% or increased by 42% (relative), p=0.41 pic.twitter.com/lyLNLVaCv4
— Covid19Crusher (@Covid19Crusher) November 30, 2021
Even more bizarrely, after Merck announced a 50% reduction in hospitalizations from the first phase of its trial announced in October, just last week the company announced that the combined efficacy is down to 30%. As some have pointed out, that raises serious concerns as to what has happened with the drug’s trial, given that the data from just phase 2 would indicate negative efficacy for the drug, with 4.7% hospitalized in the placebo group compared to 6.2% in the molnupiravir group.
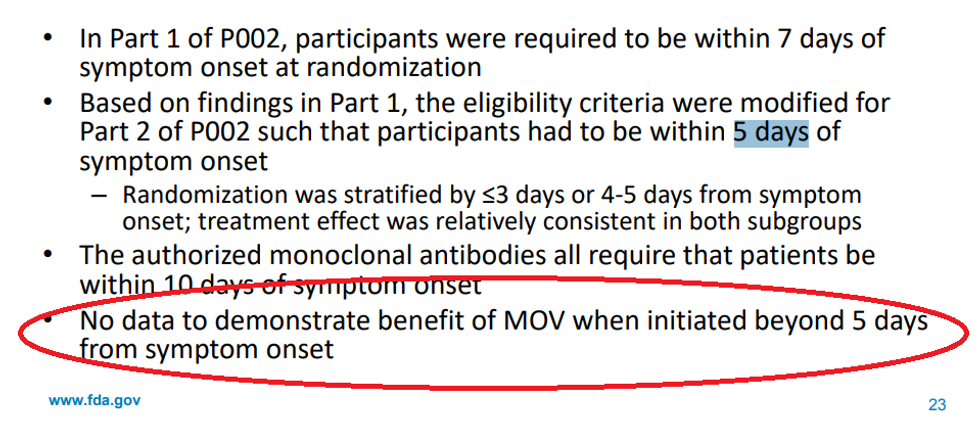
Also, remember that it has already bombed out in terms of efficacy for moderate COVID and never had the potential to work in late stages because it is not anti-inflammatory like ivermectin. The FDA concedes up front that there is zero proven benefit after day five of symptoms.
So, we are trading so much risk of injury and making the virus worse for a short window of potentially modest efficacy at a cost of $700 per person. If this is the standard for approval during an emergency, how on earth could the FDA refuse to greenlight drugs that have already established a robust safety profile for decades when independent studies from people who don’t stand to benefit show much greater efficacy and for a broader spectrum of disease at a cheaper price?
COMPARAISON IVERMECTIN (8,53€)-vs-MOLNUPIRAVIR(600€).. pic.twitter.com/shyhoVUNQU
— telephonearabe (@telephonearabe) October 31, 2021
Revision of the previous post. More precise now.
Sources:https://t.co/UHQj2wqvVThttps://t.co/ZSbtONOnUIhttps://t.co/Y4yBVV0YaNhttps://t.co/nT1o75AyHwhttps://t.co/XuQMrqsqXehttps://t.co/0Anj9lNuwkhttps://t.co/IKqkq9igJHhttps://t.co/1UaTENeeV9 pic.twitter.com/KMuNLRuOeU
— Massimaux (@masimaux) November 30, 2021
The FDA and NIH are willing to give a drug known for birth defects with low efficacy to women of childbearing age outpatient but won’t even allow a Nobel Prize-winning drug safer than Tylenol as a last resort to someone dying.
Just rinsing your nose and mouth with Betadine at the onset of symptoms or preventively works better than this drug, according to Merck’s own data.
Povidone-iodine vs. Molnupiravir pic.twitter.com/64fyTJpfGP
— Massimaux (@masimaux) October 23, 2021
Again, why would our government refuse to recommend any of these therapeutics and treatments but continue to support remdesivir and now approve molnupiravir, two dangerous and likely ineffective drugs? And what does that tell us about the process and transparency behind the FDA’s perceived safety and efficacy of the vaccines?
There are no innocuous answers to these questions.
Janet Cragan, a medical officer at the CDC and a panelist on the FDA advisory committee, bizarrely conceded at Tuesday’s meeting that “there are definite concerns about the potential effects of this drug on the embryo and the fetus,” but then said she has problems denying the drug to people! “I don’t think you can ethically say it’s OK to give this drug in pregnancy. [But] I’m not sure you can tell a pregnant women who has Covid-19 that she can’t have the drug if she has decided that’s what she needs.”
Well, how about denying the safest drugs around to everyone with COVID for the past 20 months???!!!
Roy Baynes, the Merck executive at the meeting, even had the nerve to suggest that it’s not for the FDA to tell doctors not to use the drug even in pregnant women! “But I think the idea here is that ultimately the physician is the best position to determine the relative risk-benefit for their patients,” said Baynes.
With its eight mechanisms of action against COVID and award-winning safety profile established for decades, ivermectin trounces molnupiravir in every consideration. As a 2017 article published in Nature’s Journal of Antibiotics observed, “Few, if any, other drugs can rival ivermectin for its beneficial impact on human health and welfare.” The authors noted that “ivermectin is continuing to surprise and excite scientists, offering more and more promise to help improve global public health by treating a diverse range of diseases, with its unexpected potential as an antibacterial, antiviral and anti-cancer agent being particularly extraordinary.” They fortuitously predicted, “Essentially, a unique, multifaceted ‘wonder’ drug of the past and present may yet become an even more exceptional drug of the future.” Sadly, our government is denying that future and that of several other important safe, off-patent drugs.
Anyone who can’t see the conflict of interest in this powerful juxtaposition is willfully blind to the irremediable corruption in the NIH, the CDC, and the FDA.
*
Note to readers: Please click the share buttons above or below. Follow us on Instagram, @crg_globalresearch. Forward this article to your email lists. Crosspost on your blog site, internet forums. etc.